Babyscripts has one of the most extensive provider networks in maternity care, and in the digital health industry.
Here's why more providers choose us.
Babyscripts’ first go-to-market product was created with the help of obstetricians at The George Washington Medical Faculty Associates in 2014, and since that time our providers — both users and those on our Clinical Advisory Board — have been deeply involved in the development of our product, with their feedback and insights closely guiding our product roadmap and their strategic investments showing their belief in the value of our solution. This support has translated to one of the most extensive provider networks in the digital health industry, with our provider customer base far exceeding any of our competitors in the condition-specific space.
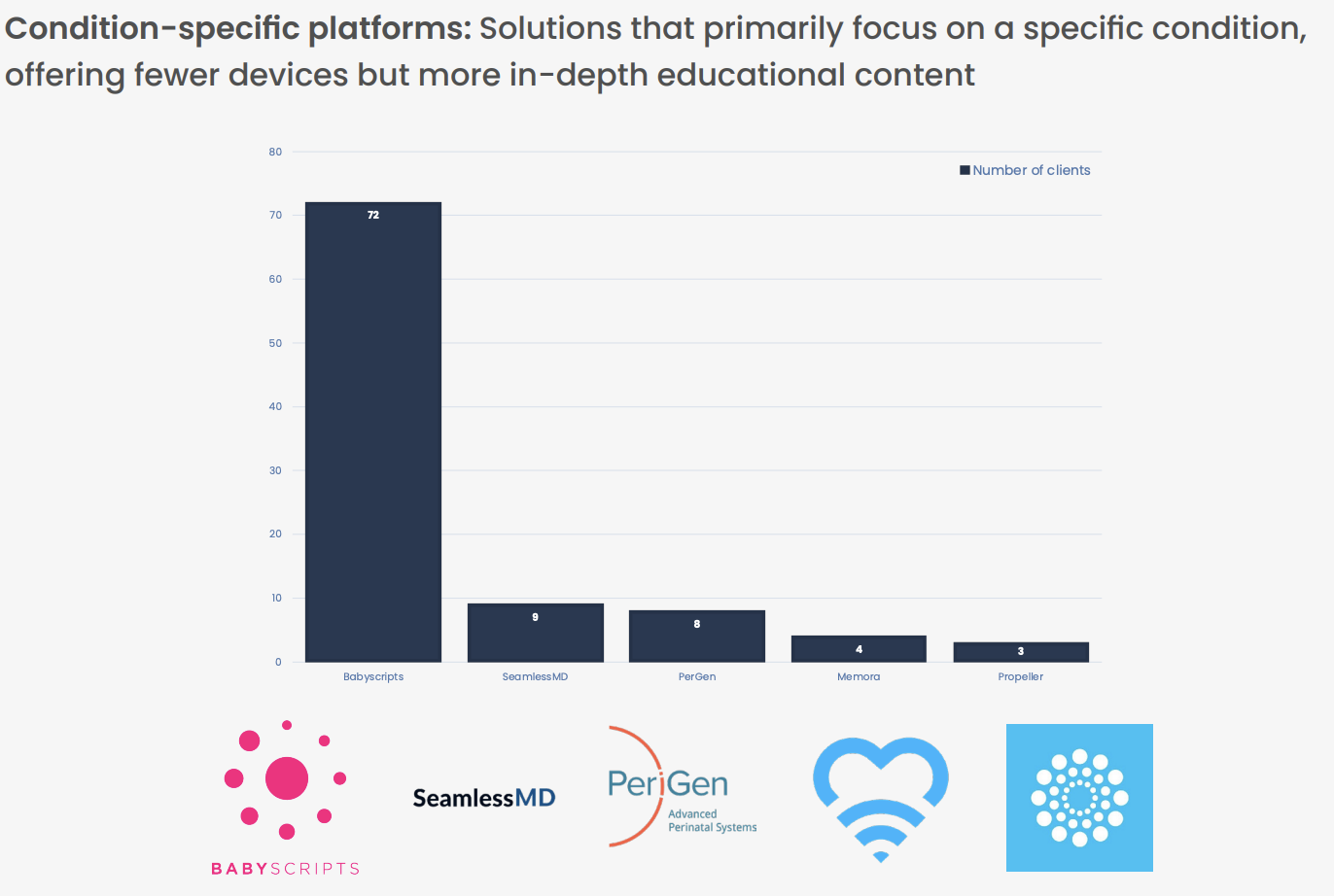
[retrieved from AVIA Connect's 2022 Remote Monitoring Report]
The original remote monitoring solution for blood pressure in pregnancy.
Unlike some other digital health offerings in the marketplace, who only began incorporating remote patient monitoring (RPM) into their solution at the onset of the pandemic, Babyscripts cut its teeth on RPM. Built with the vision to transform the traditional 12-14 prenatal care visit schedule by delivering remote care through IoT devices like our bluetooth-connected blood pressure cuff, the Babyscripts solution allows low-risk patients to attend less in-person visits without sacrificing satisfaction with care. [1]
In 2019, we expanded our solution to address high-risk patients, rolling out Babyscripts blood pressure monitoring for four separate risk categories, including normotensive, chronic hypertension, prenatal hypertension, and postpartum hypertension. While other health systems scrambled to pull together solutions to deliver care remotely during the Covid shutdown and after, Babyscripts customers were prepared with our out-of-the-box solution.
Demonstrated clinical excellence and improved outcomes.
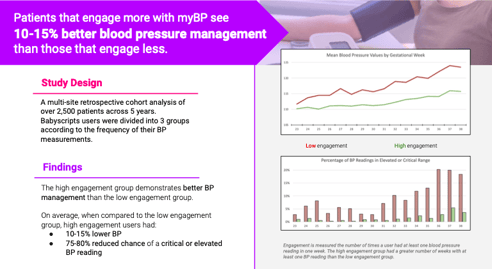
Babyscripts has been the subject of multiple studies, and the benefits of our solution are supported by a robust portfolio of research, patient case studies, and on-the-ground data. A multi-site, retrospective cohort analysis of over 2,500 patients across 5 years found that patients who engage more with Babyscripts blood pressure monitoring see 10-15% better blood pressure management than those with lower engagement rates.
In a partnership with New Orleans-based health system LCMC Health, patients enrolled on Babyscripts have demonstrated sustained compliance with blood pressure monitoring, allowing providers to capture more than four times the amount of data collected in a traditional office setting, and patient compliance with remote monitoring has exceeded the health systems target goals, with levels of patient engagement and satisfaction consistently exceeding targets by as much as thirty percent. As a result, providers were able to detect preeclampsia two weeks earlier in patients enrolled in remote monitoring through Babyscripts, compared to those not enrolled on RPM.
These users also demonstrated improved adherence to the postpartum visit attendance HEDIS measure. At 30 days postpartum, Babyscripts users were more than two times as likely to complete a postpartum visit than the control group, and at 60 days postpartum, 64% of Babyscripts users had completed a postpartum visit, compared to 44% of the control group. [2]
[Read more about our proven clinical efficacy]
Designed around OB financial incentives
Babyscripts’ remote monitoring allows providers to replace some in-person visits, opening up appointments and freeing provider time to focus on higher-risk patients, while still capturing the global fee (a model that aligns with recent PATH recommendations for reduced in-person visit schedules supplemented with RPM). With CPT codes for remote patient monitoring, Babyscripts enables health systems to maximize reimbursement opportunities, and our joint deployment model facilitates provider subsidies for Babyscripts through participating health plans.
Earlier intervention enabled by risk detection and escalation through Babyscripts can prevent negative, costly outcomes downstream, such as postpartum readmission. Even the simple efficiency of digitizing the traditional OB packet has demonstrated cost savings of up to 80%, not to mention the time saved in updating and assimilating thousands of packets per year.
Out-of-the-box solution, designed for quality and safety
As a solution designed with and for clinicians, patient safety has always been a central concern of our product development. We have fine-tuned our RPM solution alongside leading OBs over the years, ensuring the best standards of monitoring coupled with the flexibility to align it to any health system’s configurations. Our solution is aligned with fundamental national prenatal and postpartum HEDIS measures, in addition to a variety of state-specific NCQA measures, to help our customers achieve quality goals, maximize reimbursements, and avoid penalties.
Babyscripts offers an implementation program designed to stand up our solution at a customer site in a matter of weeks, including dedicated project management, collaboration with the IT team to outline and execute integration plan, and clinician training on accessing Babyscripts orders and data. Our team supports logistics around BP cuff delivery with our full service pick, pack and ship operation, and participates in ongoing collaboration to create and share custom reports for insight into customer clinical, engagement, and satisfaction goals.
Patients and providers alike have experienced high levels of satisfaction with our solution, as measured by NPS surveys and interaction with the solution.
"Patients at Cone Health are extremely happy with the experience of RPM since integration. Patients feel secure, providers have more time because everything is linked. You can monitor after hours and on the weekend when staff who might otherwise be monitoring during the week aren’t there. Patients know that we have their data. Anything that’s really urgent will be brought to us, which gives us and the patients peace of mind." - Dr. Tanya Pratt
Leading the future of OB since 2014
Over our 8+ years in the space, Babyscripts has accumulated data and feedback that has allowed us to keep our product on the bleeding edges of innovation. Our solution for postpartum hypertension anticipated ACOG’s guidance for postpartum blood pressure management and the AIM bundle for postpartum hypertension. Our solution for schedule optimization — and research supporting reduced in-person visit schedules supplemented with RPM [3] — predated recommendations under current PATH guidelines by several years.
[Read: ACOG Releases New Pregnancy Prenatal Care Recommendations]
Babyscripts’ position as leader in the space has been validated many times over, as the founders have been solicited to share their insights and thoughts on the state of the industry, as well as testify and advocate for digital health legislation on the local and federal level. Most recently, I testified before the DC Council on the positive impact of technology for managing pregnancy and postpartum care, and with the help of my team, proposed an amendment to the Postpartum Coverage Expansion Amendment Act of 2020 to mandate reimbursement for digital tools. The language we drafted appears in the bill that was passed unanimously by the Council, and it's one of the first mandates of its kind to be proposed into law.
Research summaries and original publications can be found on our website here. For more information about our outcomes, contact Babyscripts directly at info@babyscripts.com.
[1] DeNicola, Nathaniel MD, MSHP; Sheth, Sheetal MD; Leggett, Kelly MD, MHA; et al. Evaluating Patient Satisfaction and Experience for Technology-Enabled Prenatal Care for Low Risk Women [1L]. Obstetrics & Gynecology: May 2018 - Volume 131 - Issue - p 129S
[2] LCMC Health. Pregnancy-Related Hypertension: Adherence to a New Type of Monitoring
[3] Marko KI, Ganju N, Krapf JM, et al. A Mobile Prenatal Care App to Reduce In-Person Visits: Prospective Controlled Trial. JMIR Mhealth Uhealth 2019; 7(5)
Comments (1)