This month, the Green Journal published The Michigan Plan for Appropriate Tailored Health Care in Pregnancy Prenatal Care Recommendations (MiPATH), which represents the first major changes to prenatal care recommendations since 1930. It includes two prenatal care plan options based on patients' medical, social, and structural determinants of health that are built on a baseline 4-visit, in-person delivery structure, supplemented by telemedicine and remote patient monitoring.
The recommendations were presented by a panel of nineteen clinicians and researchers who represent expertise across maternity care, pediatrics, telemedicine, and social and structural determinants of health (including Babyscripts Senior Medical Director, Dr. Lauren Demosthenes), and include 1) individualizing care, 2) incorporation of telemedicine, and 3) consideration of both medical conditions and social and structural determinants of health in routine care delivery.
This is the first of several manuscripts to come out of the landmark panel. We've pulled out the key points below [read the full manuscript here].
The 12-14 in-person visit structure is outdated: one-size does not fit all.
Panelists evaluated the existing 12-14 prenatal care structure, focusing on five components: 1) visit scheduling: the appropriate timing of the first prenatal visit, first trimester ultrasonogram, and subsequent prenatal visits; 2) routine pregnancy assessments: blood pressure, fetal heart tones, weight, and fundal height; 3) the appropriateness of telemedicine for specific prenatal visits, including the use of home devices; 4) recommendations for individualizing care based on medical conditions; and 5) the effect of social and structural determinants of health on prenatal care delivery. Post-evaluation, they presented the following options for alternate visit schedules:
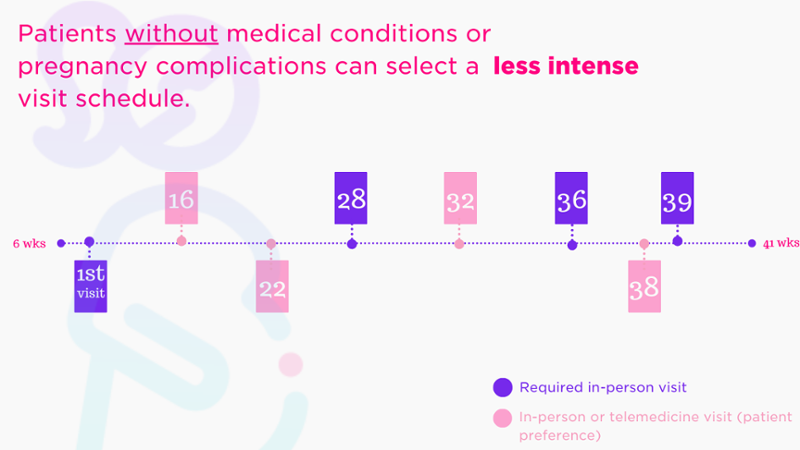
Fig. 1: Options for prenatal care plan for patients without medical risk; based on patients' medical, social, and structural determinants of health.
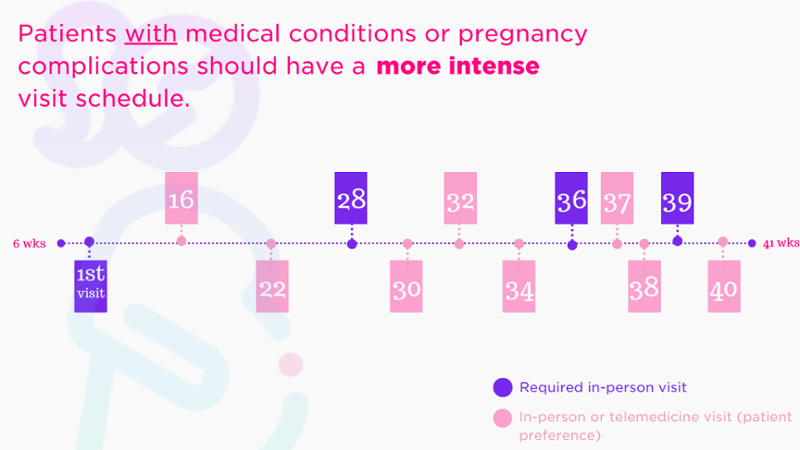
Fig. 2: Options for prenatal care plan for patients with medical risk; based on patients' medical, social, and structural determinants of health.
Social determinants of health should be a key part of risk assessment and care recommendations.
The panel worked with experts in social and structural determinants of health (SDoH) and maternity care equity to come up with a comprehensive list of risk factors, including material needs (eg, housing insecurity, inadequate health care coverage), psychological needs (eg, self-efficacy, tobacco use), social needs (eg, poor social support, intimate partner violence), and demographic characteristics (eg, immigrants, rural patients), that could potentially affect prenatal care delivery and perinatal outcomes. They agreed that a risk assessment for medical, social, and structural determinants of health should be completed as soon as individuals present for care.
Remote monitoring is appropriate for routine pregnancy assessments (and should be used more frequently for patients with existing complications, such as chronic hypertension).
The panel rated the appropriateness of routine pregnancy assessments at all (i.e., in the clinic or remotely) and remotely in each trimester, and agreed that monitoring all identified assessments (blood pressure, fetal heart tones, weight, and fundal height) was appropriate remotely and in person in the second and third trimester. Monitoring of blood pressure and weight was also considered appropriate remotely and in person in the first trimester, with encouraged frequency for patients with chronic hypertension and preexisting diabetes.
Connecting patients to additional care services can be more effective than increasing OB visit frequency.
Panelists agreed that when individuals’ identified needs could be met through additional services, the patient should be connected to these services, and that there was rarely a need to increase visit frequency beyond the average-risk visit schedule. They concluded that additional prenatal visits were not only unlikely to help address non-medical needs, but would also represent an increased burden on patients.
The panel limited its focus to average-risk pregnancies (defined as individuals who do not require care from a maternal fetal medicine sub-specialist), and in addition to individuals with no existing medical conditions, panelists selected 6 common complications for inclusion that fall under the purview of maternity care professionals: chronic hypertension; preexisting diabetes; chronic depression or anxiety; history of single prior unexplained miscarriage; gestational hypertension; and gestational diabetes.
*Since the time of publication, the Michigan Plan for Appropriate Tailored Health Care in Pregnancy Prenatal Care Recommendations (MiPATH) has been renamed PATH (Plan for Appropriate Tailored Healthcare in Pregnancy) [Updated 4.24.2025]
Submit a comment